
Post 37 Part I: This Is Why We Can't Have Nice Things. Those That Hide in the Shadows And Prevent Change Need to Be Exposed.
The field of HBOT is a microcosm of what we are seeing today - across industry, academia and medicine. Progress is being stalled for no other reason than for POWER. MAHA OR DIE, BABY.


The Pharma-Military-Industrial-Complex: PhMICkey Rat Club
* There are names that I will substitute in order to protect the identities of individuals and from being sued. One of these folks is Dr. Pat Whealler (not their real name), one of the leads in the clinical trials run by the DoD/VA/Army.
For the last 20 years, there has been a concerted effort to stop, block and slow down the acceptance of HBOT by DoD and its departments. Physician groups and other parties, aiding and abetting the federal mandate of NO HBOT, have consistently ignored the biological basis and the observed clinical reality of this medical technology. Only in the last 5 years has there been a hint of PhMICkey Rat having to alter their stance and concede any ground. If there was a will that aligned with patient interest, hyperbaric oxygen therapy (HBOT) (and other therapies) would have happened by now.
The ever-shrinking medical freedom we have all experienced (practitioners as well as patients) has been creeping slowly over us, eroding the power of the physician to act in the interest of the patient and of the patient to act in their best health interest. An example of this reality is the field of HBOT – mostly on the efforts to apply this treatment to help veterans and civilians with a traumatic brain injury (TBI), post-concussion syndrome (PCS) and persistent post-concussion syndrome (PPCS) and post-traumatic stress disorder (PTSD). This is a recounting of the behind-the-scenes efforts, counter efforts and interactions that private citizens and non-governmental organizations have had with government. This story is a reflective microcosm of our experience with the PhMICkey Rat. This story has played out across multiple fields, especially in the autism community (if you want to read about a nightmare scenario, get a hold of Andrew Wakefield’s story).
Eisenhower, in his 1961 televised farewell address to the Nation, warned the American People of the coming force that needed to be checked.
“In the councils of government, we must guard against the acquisition of unwarranted influence, whether sought or unsought, by the military-industrial complex…”
This needs to be updated to include the pharmaceutical industry – with its massive influence in the federal government and the media. The collusion of interests and the power engendered by public-private partnerships (a.k.a. – fascism) is at the heart of this story. Progress is being stalled for no other reason than for POWER. Laws and economic incentives have been altered and perverted under our noses. The only way we will get change is to become that change…and work like rented mules.
MAHA or Die, Baby.
Finding the Miraculous
In 2011, I was part of a research group on HBOT. We were part of a clinical study called the National Brain Injury, Rescue and Rehabilitation study (NBIRR) and we were recruiting active duty, veterans and civilians with TBIs. This is where I saw a string of miracles.
You really change your paradigm about science and medicine after seeing half-a-dozen people recover from TBI induced long-standing symptoms and neuro-cognitive deficits (short-term memory problems, headaches, lethargy, depression, suicidality, etc…). Reading case report after case report of people’s recovery you begin to expect the results from HBOT treatment. HBOT rarely disappoints.
One patient was striking.
A young woman, in her early twenties, suffered a head injury. The unseen type of injury, the invisible type. The type of injury that you look ok on the outside but you can feel the effects on the inside. Your ability to think, process and experience the world is affected.
She was riding on an ATV and had a roll over, knocking her head on rocks and on the ATV. She was taken to the ER, was checked out by the staff, had a CAT scan and was released to go home. No broken bones, no brain bleeds and no stiches. That’s when her troubles started. Almost from the start, she had trouble sleeping, concentrating, working and going to school. For the next year, she spiraled down into a dark hole of misdiagnosis after misdiagnosis, until she found a fourth doctor that was able to diagnose her with a TBI.
She was a straight-A college student, holding down a full course load, working two part-time jobs, and had just completed her black-belt testing in Tae Kwon Do. This person was a high functioning, goal-driven individual. In that year, she could only spare the energy and focus to barely hold on to one job and stopped going to school. Her life, as she knew it, had ended.
Her fourth doctor, which had diagnosed her with a TBI, was trying new approaches instead of giving her drug treatments to manage her symptoms. At the time we had placed an ad in the local newspapers, recruiting volunteers for our hyperbaric clinical trial. Her doctor suggested that she contact us and see if she met the inclusion criteria for the study - which she did. It had been just over a year when she got her TBI.
Not to drag out the story but when she arrived for her initial testing on neurocognitive and symptoms assessment, she was in a bad state. She almost maxed out on symptoms and her neurocognitive testing was well below the 50% standard of a woman her age. It took 3 months and 60 “dives” of HBOT but by the end of the treatment all her symptoms had resolved and she was in the +90% of neurocognitive performance. A year after starting, she was back in school (A+ in all her college classes), working her two jobs and starting a business.
She was not the only person that I observed to recover.
From my perspective HBOT is damn close to a silver bullet for TBIs. Not perfect but it gets you 85% of the way there.
And there have been several attempts to block it use. For a full story, we need to go back in time. Hang on - lots of twists and turns coming up.
Enter The Rabbit Hole
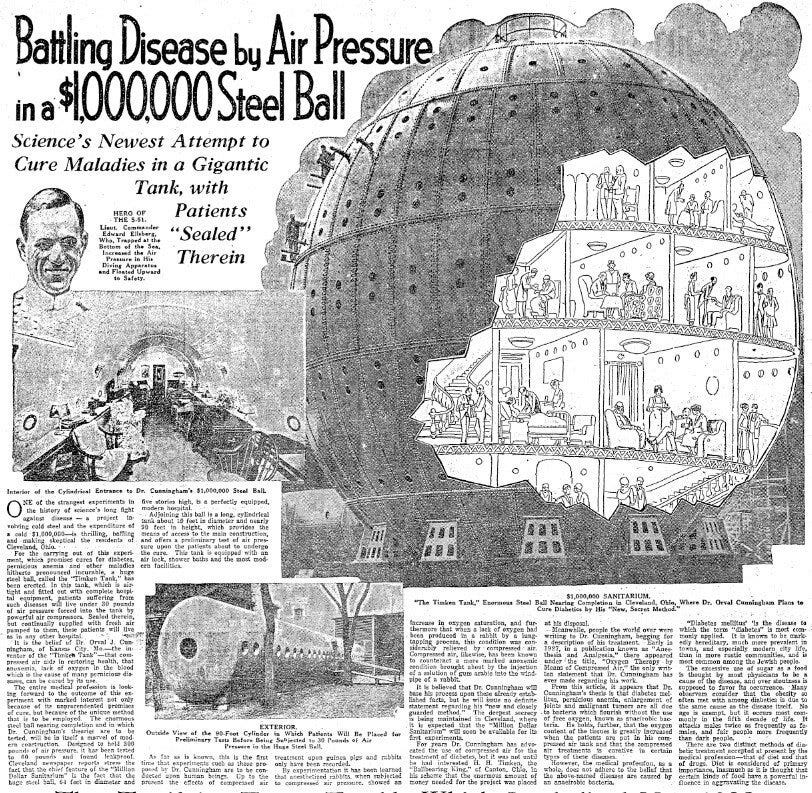
Hyperbarics entered into vogue in the 1910’s and 1920’s with a great deal of fanfare. The influenza epidemic (Spanish Flu) catalyzed the need for new approaches to treat pneumonia. Remember, antibiotics where not developed until the 1940’s.
Dr. Orval Cunningham, a chairman of the department of anesthesia at Kansas University Medical School, treated dying Spanish Flu patients with what would be diagnosed now as ARDS (acute respiratory distress syndrome), which is identical to what COVID patients experienced. The parallels with the Spanish Flu are uncanny with today’s plandemic BS. As you can imagine, news of these treatments got a lot of play in radio, reel and print.
Due to early success, Dr. Cunningham expanded his practice to treat other conditions. It was this early success that drew attention and financial investment in a bigger treatment space. It also drew the Eye of Sauron (the Malochio or evil-eye) onto him and his practice from the American Medical Association (AMA).
The AMA was founded in 1847 and incorporated in 1897, becoming the largest association of physicians, including both MDs (Medical Doctors) and DOs (Doctor of Osteopathy) in the United States. The mission of the AMA was to “promote the art and science of medicine … promote public health and lobby for legislation favorable to patients…”. The AMA also lobbied for laws requiring compulsory smallpox vaccinations (1899), similar to what had transpired in the UK decades earlier – under the progressive era banner of “hygiene”. At the time, the vaccination mandates against smallpox had zero levels of actual evidence of efficacy – vaccination being a theory with scant clinical or public health support at the time – the AMA felt sufficiently justified to promote.
In 1919, medical practice was not as codified and structured as it is today. The AMA in 1904 had established the Council on Medical Education (CME), whose objective was to restructure American medical education and the practice of medicine. In 1908, the AMA (via its CME) was hell-bent on reforming medical education and practices – ostensibly for the “public good”.
The AMA contracted with the Carnegie Foundation for the Advancement of Teaching to survey the American medical education system. The Flexner Report was published in 1910, providing a Prussian-pedagogical perspective on the status of medical education in the United States and Canada, under the aegis of the Carnegie Foundation. These reforms led to the elimination of schools that failed to meet allopathic and osteopathic “scientific” standards of the day.
Thus, the AMA set the standard for what it considered “credible” medical treatment. The conflict of interest between the Robber Baron Foundations of the era and the soon-to-grow AMA cannot be over-emphasized. The AMA set the standard and the Carnegies and Rockefellers used their endowment to direct the formation of school boards (buying doctors) to “reform” medical education. These changes certainly set standards for medical schools - and eliminated the rapidly growing field of naturopaths and homeopaths. It also created a lucrative market for petroleum-based, chemical feedstock to make drugs - which could be funneled to a new and growing base of prescribers.
Cunningham, using his professional and clinical experience, expanded the use of HBOT to treat conditions like stroke, heart disease and dementia. With success stories increasing, more and more patients reached out to him for treatment. As his fame grew, it drew the attention of the AMA - which launched an investigation on his claims of treatment in 1921. Mind you, the AMA had not received any complaints from patients - it was “concerned” about the amount of money that was being made by Cunningham with “unproven” claims. The flagship journal of the AMA, JAMA, began a campaign against Cunningham and “invited” him to show his evidence for treatment. Cunningham declined the invitation and did not go on the offensive, ceding the ground to AMA attacks.
By 1928, due to continuous attacks in the newspapers and threats of lawsuits, Cunningham sold off his practice. By 1929, the Great Depression hit. By 1936, the entire center was sold off at auction. This one event greatly colored the credibility of HBOT in the eyes of the emerging medical education environment and medical practice.
The AMA NEVER received a complaint about Dr. Cunningham over the practice of medicine. Just a vague allegation from a family claiming that Dr. Cunningham was charging more than they could afford. No evidence of malpractice or withholding of treatment.
Does it sound familiar? Shades of Ivermectin and state medical boards.
Since the Cunningham event, HBOT was tainted with the quack brush. Yet, over the decades, numerous doctors and surgeons explored the potential of this medical technology in the rising cases of cardiovascular disease, the new scourge of modern society. Early work was showing that it was an effective agent for stroke recovery and aiding in survival of complex surgeries. Unfortunately, if you could not afford a large, multi-place chamber (like big hospitals or universities), you could not do these types of investigational studies.
With the advent of small mono-place hyperbaric chambers, MRI and SPECT imaging, the ability to treat emergency victims and measure blood flow and oxygen uptake in organs (including the brain) allowed for objective measures and new ideas to be tested. Work by doctors like Neubauer, Maxfield, Harch and Rockswold demonstrated that severe traumatic brain injury (sTBI) responded exceptionally well to HBOT. Rigorously controlled, randomized human clinical studies showed as much as 60 percent reduction in total mortality in sTBI patients receiving HBOT, compared with standard intensive care without HBOT. Yet, HBOT is not approved for sTBI - even when it saves lives, reduces costs and spares mental and physical function. HBOT is treated like the Rodney Dangerfield of medicine - It Can’t Get No Respect.
Recent studies have shown even more impressive improvements along a whole slew of metrics. But, when there are people (or special interest groups) that don’t want the game to change, roadblocks are always put up to slow progress or kill change.
As always, when the times demand it, patriots step forth.
Good Public Servants Are True Patriots
Enter Mr. Martin (Marty) Hoffmann - I will need to provide some background on this unique and incredible individual. He enlisted in the Army after graduating from Princeton University in 1954. Prior to accepting his commission after Officer Candidate School as a 2nd Lieutenant, he had achieved the rank of Sergeant. He was released from active duty in 1958, with the rank of 1st Lieutenant and stayed on as member of the Army Reserves. He became a practicing lawyer in the interim and was selected as the general counsel for the Atomic Energy Commission in 1971, under the chairmanship of Arthur Schlesinger. President Ford nominated Mr. Hoffmann as Secretary of the Army, which forced him to resign his commission as a Major in the Army Reserves.
Martin R. Hoffmann was appointed as Secretary of the Army from August 5, 1975 until February 13, 1977. He oversaw the transition of the Army into an all-volunteer force, as the Vietnam War was winding down. Mr. Hoffmann’s belief that continual improvement of the soldier/service member in all aspects of the experience was an essential goal for the Army. At the time, Mr. Hoffman was seeing and hearing of a new syndrome associated with returning Vietnam veterans - post-traumatic stress disorder (PTSD). As Secretary of the Army, Mr. Hoffman was continually flogging the Army to investigate this as a medical condition for coverage and treatment. As much as Mr. Hoffman pushed, the DoD slow-rolled him for his entire time as Secretary until Ford was out of office. With a new administration, Mr. Hoffman was asked to step down. It would be decades later that PTSD would come to the forefront again.
Mr. Hoffman became an advisor to Defense Secretary Donald Rumsfeld in 2001. One matter that captured his attention until his death was the recognition of traumatic brain injuries and PTSD in Service Members. The rate of injury of this type was (and is) rampant and was not being addressed or recognized within military service. When he saw the reprise of the PTSD problem with TBI post Iraq he pursued this with the intent of not allowing the Army/DoD to ignore it as they had done with PTSD. He actively lobbied for recognition of this injury and to speed up development of diagnostic technologies and treatments. He, along with many Veteran and civilian supporters, pushed for and obtained funding to begin trials on novel therapies to treat brain injuries. One of the therapies he pushed for recognition within the Army was hyperbaric oxygen therapy (HBOT).
He believed that the Army has a duty and responsibility to treat their injured and restore them to health, prior to releasing them or the Service Member separating or retiring from the military service.
As he learned, post his career as the Secretary of the Army, HBOT was an effective treatment for TBI and he wanted to make the Army (and the Department of Defense, by extension) aware of this technology. This reminder of duty was coming from a former Secretary of the Army, a former Service Member (active and reserve) and not an idealist. The journey from public servant to persistent patriot continued down a very, very windy road.
The Political Is Personal
Marty worked for the State Department during the early stages of 2001. After the US Coalition entered Afghanistan, Marty was involved with the political and government infrastructure rebuilding of Afghanistan. To help with the job he recruited a dear friend and colleague, Judge Pat Maney, working in Florida. Brigadier Army General (Reserves) Maney was recruited to coordinate and administer the reconstruction in Afghanistan. While in-country he is blown up in his armored Humvee.
General Maney survived but suffered very significant neurocognitive deficits and was racked with severe neurological symptoms - classic and easily diagnosed traumatic brain injury. He was sent to Walter Reed where he wanders the halls of the premier Army hospital for 12 months, getting whatever therapies they had to offer. Marty frequently visited Maney at Walter Reed. He watched him wandering around in his hospital pajamas - aimless and unaware.
Pat Maney was rendered mentally and physically unable to continue his duty and to return to work as a state judge. The experts at Walter Reed told him this was his new normal and only “the tincture of time” had the possibility of returning him to full capacity- if ever. Now, this is where fate steps in to intervene and closes a few loops.
Pat Maney’s family friend in Fort Walton Beach, FL is Dr. Eddie Zant, a hyperbaric physician. Now, Dr. Zant is a doctor’s doctor - he will do what he has to in order to treat his patients and get them better. Dr. Zant had heard that a fellow hyperbaric physician was having success with HBOT on neurological conditions. Dr. Zant and his wife contacted Pat Maney’s wife (Caroline) and gave her a copy of the “experimental protocol” that had been in development and testing since 1989.
Caroline Maney dutifully approached Maney’s colonel at Walter Reed and provided the HBOT protocol for review. The previous 12 months had not delivered any improvements in his condition, so there was nothing to lose, except more time. Fortunately, the good colonel agreed to try this “experimental” therapy and he was sent to the closest hyperbaric chamber in the D.C. area - George Washington Hospital. It was there that he received 80 HBOTs dives in two blocks of forty (2008) treatments.
Now, Marty Hoffman, the good friend of Pat Maney, regularly went to visit and spend time with his friend. Marty was beside himself when he saw Pat, previously a shell of his former self, back to the way he remembered him before the accident. Gen. Maney was discharged from Walter Reed, fully recovered from his neurological deficits and symptoms after 3 months. He returned to his judgeship in Florida, which he continues to this day. The old, ass-kicking Secretary of the Army persona kicked in and asked the doctors at Walter Reed, Pat and Caroline, “How did this happen?”
When he heard that it was HBOT, Marty wanted this for every service member with TBI. If you are not getting the picture now, Marty was an action-oriented individual that did not take NO for an answer.
After Marty did some checking around (who the hell developed this protocol?), Paul Harch (M.D.) got a phone call. In short order Marty was in New Orleans on Canal Street at the Sheraton Hotel having breakfast with Dr. Harch, getting the full run-down on the success they had been having treating TBI patients for the past 9 years.
As Dr. Harch and Mr. Hoffman were conversing on Canal Street in 2008, a history of side-stepping and active ignoring was exposed. Previously, Bill Duncan (Ph.D.) and Dr. Harch had attempted to get the governing body for medical training in hyperbarics (the Underwater and Hyperbaric Medical Society, UHMS), DoD and Walter Reed to begin testing HBOT on TBI diagnosed service members.
As a starting point, Dr. Harch recounted the early efforts to make Army Medical aware of a potential treatment for TBI. An ex-roommate of Dr. Harch (from medical school), now a colonel in the Army (Dr. John Jaffin) made the introductions to the staff at Walter Reed. Walter Reed is the premier Army medical hospital for rehabilitation.
The data for effectiveness of HBOT was presented to the PM & R Department and the Medical Director of Walter Reed in 2004. The presentation ended with Dr. Harch offering to treat, FOR FREE, any and all service members that were diagnosed with TBI, post-concussion syndrome (PCS) and/or PTSD.
The Medical Director for Walter Reed refused.
This was at the height of the Iraq and Afghanistan conflict, with improvised explosive devices (IEDs) injuring and debilitating our service members and creating the invisible wounds of this conflict. We were stacking up a very large backlog of TBI and PTSD injured service members.
Dr. Harch and Dr. Bill Duncan (former staffer of Rep. Istook, OK) had been all over Washington, D.C. for over six years. Congressman Istook used his influence to get them in and have face-to-face talks with head of federal departments. The duo went about showing SPECT brain scans (an imaging technology that allows you to see the metabolic activity of the brain) of TBI patient treated with HBOT to government agency heads. The images clearly showed great improvement in cerebral metabolism that coincided with symptom reduction, improved neurocognitive performance and improved quality of life. This went on for several years as a lobbying effort to get HBOT recognized as a POTENTIAL treatment. All that was needed was a little bit of funding - the equivalent of budgetary lint from the purse. Little happened until Marty got involved.
As Dr. Harch conveyed the history that he had with getting HBOT integrated with Army and DoD, Marty slammed his fist on the table and said that he didn’t want to hear “any of that bullshit”, he wanted this now for every injured service member. Dr. Harch told Marty that he would be happy to have him lead the way with the DoD.
Now aware of each other’s previous experience, they began to work in unison in 2008.
PhMICkey Goes Offensive - Rat-fuckery A-plenty
By the Spring of 2008 Duncan and Harch had been going for 7 years to get the DoD interested in HBOT. One project proposed to the DoD was to install a multi-place chamber in Iraq to treat acutely injured service members with HBOT. The proposal was based on well-established HBOT indications for burns, crush injuries, air embolism (blast), acute traumatic peripheral ischemia - all diagnosable in a TBI. None of these indications were considered experimental. The proposal failed after multiple yearly attempts to get it into the DoD budget.
At a D.C. party in the spring of 2008 Duncan sidled up to the Secretary of the Navy who confided to Dr. Duncan that the Navy/Marines had a significant problem with TBI-injured Marines and had no solution. Duncan suggested HBOT and the Secretary had the Navy Surgeon General (Admiral Robinson) invite Dr. Harch to present his experience at the Bureau of Medicine and Surgery in D.C. in August 2008. Present was the Navy Surgeon General, the Asst. Commandant of the Marine Corps, Duncan, Marty Hoffmann, U.S. congressional office representatives, the wives of the Joint Chiefs of Staff, Navy doctors, and other VIPS, along with 4 of the veterans Harch had treated with HBOT for TBI who gave testimonials.
Harch’s presentation started off with a straight-forward request: ask for funding for a study. Admiral Robinson told Harch, “Dr. Harch, funding is the least of your problems. I have $900 million dollars in research allocated to my budgets.” Both Admiral Robinson and the Asst. Commandant repetitively nodded in approval during the presentation, indicating that funding was a done deal and they were eager to move forward.
At the conclusion of the meeting Robinson asked Harch to work with his team of doctors and experts to move HBOT forward for brain-injured service members. Harch agreed and began submitting literature to help the Navy docs understand HBOT and HBOT for TBI. During this time period, a separate group within the DoD and USAF had initiated a protocol to test the effects of HBOT on active-duty personnel. The ostensible lead of the study (and the initial designer of the treatment protocol) was Dr. George Wolf.
Side bar 1: The USAF study would be published in 2012 (The Effect of Hyperbaric Oxygen on Symptoms after Mild Traumatic Brain Injury, JOURNAL OF NEUROTRAUMA 29:2606–2612 (November 20, 2012)) and would become one of three studies used to recommend against the use of HBOT. Dr. George Wolf was the lead author and P.I. - but it would later be disclosed that Dr. David Cifu was the author responsible for altering the manuscript and minimize the objections and discussion of outcomes that Dr. Wolf attempted to publish. More on that later…just keep it in mind.
The first thing that the Navy Medicine docs asked Dr. Harch to do was review the study design that was proposed at Brooks Air Force Base (see Side bar 1). The study design had an air treatment group (1.3 ATA) that was going to be used as a control (the assumption being that pressurized air is not biologically active - 100% wrong) and a 2.4 ATA, 100% Oxygen group.
Dr. Harch informed them that 2.4 ATA was too much (normally used for ischemic limb or wound management) and there was no evidence of its effectiveness in chronic mTBI. Moreover, it carried a risk of O2 toxicity, a condition that primes the central nervous system to trigger seizures. Admiral Robinson’s group ignored the medical literature review initially, finally responding to Dr. Harch’s queries after repeat emails. The admiral’s medical leads told Dr. Harch that it was his responsibility to inform the folks running the HBOT study at Brooks AFB of the risks.
Dr. Harch dutifully sent an email to the director of Brooks AFB, Dr. Cheung, in San Antonio. No response was forthcoming from the director at Texas. The zeal and interest initially shown by Admiral Robinson’s group went to nothing and zero funding was forthcoming.
Slow Rolling and Ear Tagging the Troublemakers
A conference was commissioned by Admiral Robinson and scheduled for December 2008 to purportedly hear and see “Harch’s case experience so far” and the science of HBOT in TBI (Consensus Conference on HBOT in TBI). Let’s remember that it was August of 2008 that Dr. Harch and Dr. Duncan had managed to get a foot in the door with Navy Medicine. Only four months had passed since the meeting at the Bureau of Medicine and Surgery in D.C.
The Consensus Conference (December 5-6, 2008) was set in Crystal City, Virginia, in line of sight of the Pentagon – just in case anyone got any ideas. The conference was set up, ostensibly, by the Navy but administratively it was managed by the UHMS - the professional society that set the standards and training for hyperbaric medicine - increasingly behaving as an agent for the DoD and carrying water for the end goals of the program to stall HBOT. As Harch and members in attendance were coming to realize, this was a conference to slow walk the clinical science of HBOT to treat TBI and make it look like a fair hearing was being given to this treatment.
Side bar 2: Dr. Harch had been a member in good standing at the UHMS, an organization that ostensibly fights to educate and advocate for their members and the benefits of HBOT. You would think that there would be an active program to promote and fight for the expansion of its use and demand for insurance reimbursement for services and activities rendered. The UHMS leadership expelled Dr. Harch because he continuously pushed the leadership to add TBI as a treatable condition, using the acceptance criteria set forth by the UHMS committee. The UHMS, confronted with scientific evidence that HBOT was a treatment for brain injury, changed its acceptance criteria on the spot and expelled Dr. Harch from the UHMS. Complaints and charges were filed by the UHMS leadership as the excuse to get Dr. Harch out. Pure politics - or as I like to call it, Consensus Science.
At the end of the Consensus Conference, Brig. Gen. Dr. Loree Sutton, head of the DoD Center for TBI and Psychological Health pulled Dr. Duncan, Dr. Harch, Dr. Mozayeni (long-time collaborator in HBOT in the D.C. area) aside. General Sutton was aware of the effectiveness of HBOT for neurological conditions. Ten years prior to this meeting Harch helped General Sutton prepare a white paper on the effectiveness of HBOT on cerebral palsy for the Army Surgeon General’s Office.
The writing was on the wall and the Navy and Marines were not receptive to the idea that an effective TBI treatment was possible with HBOT…money was not forthcoming for an independent, civilian, third-party study. This was a program to deny treatment by labeling it as ongoing clinical research - blocking the possibility for the next 10+ years.
General Sutton told the gathered researchers that the current plan by the Navy was unacceptable to the DoD and flew against her duties as the head of the DoD Center for TBI and Psychological Health. She wanted to know how soon the gathered team could start treating troops. On the spot, a map was drawn of the U.S. on a piece of paper and General Sutton pointed to all of the Army Wounded Warrior troop locations and queried the doctors as to the HBOT resources that were close to the Army Wounded Warrior troops. Sutton wanted a plan to begin the treatment of wounded warriors with TBIs, using a structured protocol approach so that data could be gathered while troops were getting treated. Sutton told the gathered trio to develop this plan without any concern for money. She would be calling to schedule a meeting. On Christmas Eve General Sutton called Bill Duncan to gather the team and to be in Washington on 1/9/2009. Things were looking up and a path forward was becoming a reality.
On 1/9/2009 the group gathered in Washington at a secure unmarked office complex (Harch, Duncan, Beckman, Marty Hoffman and General Sutton). Col. Williams was invited to attend via phone (Col. Williams was an Air Force neurologist who was the head of the Consensus Conference and open to new ideas) and the protocol and planning was discussed to implement HBOT for TBI. Sutton appointed Dr. Harch as the P.I. for ALL of the DoD’s research projects on alternative therapies for TBI and PTSD, especially HBOT. A budget of $25 million was estimated to run the research and all the protocols would be ready in a matter of weeks. The mood was positive and the outlook bright.
Four days later Bill Duncan received an email from General Sutton, telling the group that they would not be involved with the DoD in any capacity. General Sutton informed Duncan that she had been told that the DoD was stopping this project “due to outside influence and undue bias” from these civilians. It all amounted to a hill of bullshit - orders came down to stop the honest efforts of independent researchers from getting in the way of the narrative that was forming around HBOT: “It Doesn’t Work - Stop Asking to Use It!”
Within days Capt. Brett Hart, U.S. Navy active-duty diving doctor and UHMS luminary called Dr. Harch’s office and home multiple times demanding that he put in writing everything that had been presented at the Consensus Conference. Dr. Hart assured Dr. Harch that the DoD was moving forward with HBOT TBI studies. Dr. Harch, realizing that this was part of a plan to kill the idea of HBOT, refused to participate in a farce and a crime against the wounded service members.
Dr. Harch’s concern with the group within DoD, Navy, USAF and VA, suggested to a hidden motive for the request. It seemed more plausible that they wanted plausible deniability – essentially to state that they took the recommendations of HBOT “advocates” and tried to duplicate it but failed. This concern would be borne out several years later by deeply flawed published studies of Wolf (2012), Cifu (2014) and Miller (2014), publications that would be used to justify not using HBOT to treat service members.
Months later, one of the few leaders within DoD willing to act (Brig. Gen. Loree Sutton) was relieved of command. The escapade with HBOT helped grease the skids to oust General Sutton and to quash internal leadership that was not sticking to the narrative DoD wanted out in the world. Drugs and future therapies (that the DoD wants to support or control) will be used. Until then…pound sand.
Ideas Are Bullet-Proof…They Just Hurt When They Get Hit
Even though groups within the DoD did not want to investigate HBOT, the real world was forcing the issue. General Pat Maney (Marty Hoffman’s friend) had been treated successfully with HBOT. Hard to ignore a Brigadier General that went from near-vegetable to a fully functional state judge.
In 2009, the first case reports of HBOT being able to address the symptoms and neurocognitive deficits of active-duty military service members with a mTBI were published. Two papers rattled the cages at DoD, keeping this therapy front and center.
A comprehensive and unique case of TBI (also diagnosed as post-concussion syndrome) and post-traumatic stress disorder (PTSD) was diagnosed and resolved using HBOT. This was accomplished with objective measures of cerebral blood flow improvements.
A 25-year-old male military veteran, diagnosed as suffering from post-concussion syndrome (PCS) and post-traumatic stress disorder, from an explosion in combat. The patient underwent HBOT and experienced a permanent marked improvement in his post-concussive symptoms, physical exam findings, and brain blood flow. In addition, he experienced a complete resolution of post-traumatic stress disorder symptoms. This was three years after his injury and diagnosis (Low pressure hyperbaric oxygen therapy and SPECT brain imaging in the treatment of blast-induced chronic traumatic brain injury (post-concussion syndrome) and post traumatic stress disorder: a case report).
An active duty clinician for the USAF, Dr. James Wright (Col., Air Force) and his co-authors, were also publishing the outcomes of successful interventions on two more service members (Case report: Treatment of mild traumatic brain injury with hyperbaric oxygen).
Two Air Force truck drivers were exposed to IED blasts. Both did not suffer any outwardly visible injuries but they started spiraling down with debilitating symptoms (headaches, sensitivity to light, memory problems, mood swings). They were about to get medically discharged from the Air Force when Dr. Wright intervened and delayed the medical board. He treated both airmen and they made full recoveries. The medical board did their review and cleared both men back into active duty (which is what both airmen wanted). So, clear and direct evidence for a clinical benefit was present early on and support for HBOT was building.
Two independent physician groups and three service members experience long-lasting improvement and relief of symptoms with HBOT. No drugs, no side effects, a return to a functional life and reduced costs for the VA and the community. Win-win, right?
Marty (as well as other veteran patriots) had been working for years in the US House and Senate to educate legislators on HBOT and the looming TBI crisis that was about to burst forth. At a minimum, they wanted funding for a clinical trial (in veterans) to test if a clinical benefit was present with HBOT treatment - $1.2 million was the cost to run a clinical trial.
While the lobbying was going on in 2007 and 2008 for an earmark, a self-funded TBI study on veterans was begun in the fall of 2008 with the help of Duncan and Marty Hoffman. An initial group of 6 veterans were treated pro bono at Harch’s HBOT clinic in the spring and summer of 2008. These 6 veterans served as foundational cases to develop the clinical trial protocol that was being planned.
The DoD had told Harch that his past TBI cases were not applicable to veterans and he needed veteran pilot data (what part of veteran does the DoD NOT understand?). Duncan, Marty, and Harch raised $643,000 over 4 years (2008-2012) to fund the study done in Louisiana, known as the LSU Pilot Trial of HBOT in TBI veterans. The first large gift came from the Marine Corps Foundation - the Marine Corp wanted action to treat their wounded. Interest and optimism were present from the start due to the promising pilot data results.
After the first donation came in, the Marine Corp Foundation unexpectedly refused or declined to make any more donations. Sources close to the Marine Corp Foundation revealed that the leadership (civilian, active-duty and veteran) had been threatened with punitive actions by government/military sources should they make any more donations. Meanwhile, the DoD threatened Harch saying that it was illegal and unethical for him to treat veterans (which regulations/statutes were being violated?) and similarly threatened active duty servicemembers from participating or receiving treatment since it was the acceptance of a monetary gift exceeding $25 or $50 (whatever the minimum level was) - nice little Catch-22 on the DoD’s part.
Regardless of the roadblocks and interference being thrown against Hoffman, Harch, Duncan and Mozayeni, their efforts in Congress in 2009 resulted in an Earmark that would be administered via the Army's department of research and material command (DRMC) for the clinical trial at Louisiana State University (LSU). The $1.2 million that was needed to run the study was granted.
Placing The Thumb On The Scale
As the fiscal year (2009) was winding down there was zero communication from the Army's DRMC. No money had been released to cover the cost of the study. The research team had spent and borrowed their own funds to get the clinical trial going. Both Dr. Harch and Mr. Hoffman directed multiple inquires to the DRMC. The DMRC replied that they could not locate the $1.2 million in funds.
Yup, I’m sure you are shocked at the development.
DRMC dragged the release of the funds to the final day of the fiscal cycle, at which time the monies would get absorbed by the DRMC for their use - they could then do whatever they wanted to do with the money.
It was only due to the intervention by Louisiana Senators and Congressman on behalf of Dr. Harch and Mr. Hoffman, threatening the DRMC administrators and commanders of the Army, that if they did not release the funds THEIR heads were going to roll. All of this occurred in the very last day of the fiscal cycle. The money was released on the very last day.
The LSU HBOT study proceeded to treat 16 veterans, until funding ran into a blackhole. The lack of additional funding was timed just right to force the presentation of the first half of the data at the 8th World Congress on TBI in Washington, D.C. on 3/12/2010. Dr. Harch’s presentation was on a Friday, at which time Dr. Harch had to leave. On Sunday, Dr. Duncan, Dr. Mozayeni and Marty Hoffman had a sit-down meeting with the Surgeon General of the United States Army & Commanding General of the United States Army Medical Command, Eric B. Schoomaker. General Schoomaker specialized in the field of hematology - having zero experience or background knowledge on hyperbaric medicine. By his side was another Army medical doctor (Pat Whealler), his subordinate. Both had attended Dr. Harch’s presentation. Schoomaker proceeded to inform the gathered members at the private meeting that the data that Harch just presented was all placebo effect.
How Schoomaker arrived at that conclusion is beyond me. It smacks of confident ignorance, a deep lack of knowledge of the field or a predetermined bias to ensure that HBOT would not get approved. Either way, one of the (if not THE) top medical officers for the US Army did not want HBOT approved.
One of the most damning aspects of the behavior from the Army’s top medical leadership is the fact that the Army had the therapy in-house and it was approved in the Textbook of Military Medicine (Conventional Warfare: Ballistic, Blast, and Burn Injuries: Textbook of Military Medicine Series on Combat Casualty Care, Part 1 Vol. 5, P. 313; Ballistics, 1989) as a treatment for neurological abnormalities of blast casualties. The US Army Medical Command was ignoring its own information - actually, it was actively delaying any recognition of a treatment for TBI and desperately trying to discredit any studies of HBOT. (Thank you to Mr. Tom Fox [Maj, ARMY, ret] for pointing this kernel of truth out to me).
Hell, they were actively funding and running their own studies to muddy the waters. What’s worse, they were running interference to stop or coerce researchers in the US from doing or publishing their own clinical research.

The All-Seeing Eye of the DoD
As Hoffman and Harch (and plenty of others) were discovering, the DoD/VA/Army was pulling all the stops to block any good press for HBOT. Harch had been very open about his clinical trial. On November 2011, he published the first 16 patients (out of 30 total) treated with HBOT, with OBJECTIVE measures of blood flow improvement in the brains of the TBI-diagnosed veterans (A phase I study of low-pressure hyperbaric oxygen therapy for blast-induced post-concussion syndrome and post-traumatic stress disorder). Objective measures are hard to counter, as they constitute physical evidence with little in the way of interpretation. Although the Pentagon was aware of the research being done by Harch and crew, the full glare of The Eye of the Pentagon came full force - this paper needed to be stopped or discredited.
Prior to getting the paper published, the DoD sent groups to investigate Dr. Harch at his LSU facility and demanded to get a preview of the results. This was a significant chunk of data, including thousands of SPECT images (3D models of cerebral blood flow and cerebral metabolic activity). Dr. Harch, being a respectful researcher and colleague, obliged the representatives of the DoD. The only conditions that Harch applied was to request (the Army obliged) and send their top neurologist (Col. Dr. Jeffrey Link), their top clinical trials specialist (Col. Dr. Miller), their finest imaging specialist, and finest neuropsychologist. Since all were all on the same team (in theory) wanting the best outcome for the injured service members - showing them the results was the right thing to do (which took days).
After the initial review, the DoD group insisted on being a part of the analysis team - which meant a data sharing agreement - and a potential legal and publications battle if they were invited as authors. They persisted in trying to get access to the results, including offering to run the statistical analysis of the data. If Whealler and his team had been invited to be a part of the publication, they could have scuttled the paper in a hundred different ways. Dr. Harch refused. A wise decision in my opinion…the manuscript and research were the responsibility of Dr. Harch and his team.
When the first half of the study was published online in the Journal of Neurotrauma, Whealler sent a disturbing email to Harch asking him if he had notified the journal that he was only publishing half of his data. Harch immediately called the journal to confirm that they were aware that half of the study had been completed (in the article it stated that this was preliminary evidence). They assured Harch that they were well aware that this was a pilot uncontrolled study and that this was the first tranche of data so far completed.
Whealler then contacted the editor, Dr. Povlishock. As the story was conveyed to me, Whealler repeatedly threatened Dr. Povlishock with loss of his credibility and the credibility of the journal if they didn't retract Dr. Harch’s article. Apparently, Whealler even stated that because they had seen all of the data, the paper was reporting just the first half of the data. Whealler insinuated that the second half of the data was negative such that the initial publication was fraudulent. This was a misrepresentation, if not an out-and-out lie.
Sidebar 3: At a meeting in New Orleans, requested by the Army Surgeon General’s Office and Whealler, Harch had shown them all of the data in the 2012 publication of the first 16 patients. Additional data with the next 10 subjects were presented, all with statistical analysis that showed even clearer and significant results. The only data remaining that Whealler’s team didn’t see was from the final 4 patients and Harch informed them that he had seen the data and it was consistent with and equivalent to the data of the 26 that he presented.
Dr. Povlishock told Whealler that they had investigated Dr. Harch extensively, and unless Whealler could prove that Dr. Harch and the manuscript was a fraud, they would publish it. At this point Whealler paused and apologized to Dr. Povlishock - I am paraphrasing here - “I have never done anything like this…I had to do it. I apologize.” Whealler hung up.
Wait…It Gets Better
This was not the last attempt by the DoD/Army/VA to scuttle or obfuscate the research with HBOT on TBI. In November, 2012 the Wolf study (see Sidebar 1) was published - almost a year after Harch’s paper on the 16 veterans. The day it appeared online Harch saw the article and was shocked to find out that it had been uploaded with text only: no figures, tables, graphs, data. None. Harch immediately emailed and called George Wolf to alert him of this error and to request that the remaining data be uploaded.
Dr. Wolf said he had not seen the upload. Furthermore, Dr. Cifu (one of the authors on the paper) was responsible for this the manuscript. He stated that he (Dr. Wolf) was not in charge of the content of the article despite being the lead author and P.I. -
Per Dr. Wolf: “Cifu wrote the article and was the corresponding author.” Dr. Wolf informed Harch that he was no longer in control of the manuscript. The paper concluded the following:
“Given that HBO2, in this controlled study, demonstrates no therapeutic value, requires long treatment series, is expensive, exposes patients to potential side effects, and has limited availability, clinical usage is not warranted for the management of symptoms of chronic mTBI at this treatment pressure.”
Harch informed Wolf that he would write a letter to the editor, pointing out the flaws and invalidating the paper itself (Harch’s letter to the editor is a methodical dismantling: Hyperbaric Oxygen Therapy for Post-Concussion Syndrome: Contradictory Conclusions from a Study Mischaracterized as Sham-Controlled). Dr. Wolf was in full approval and support of Dr. Harch’s critique. To this date there is no published defense of the article by the authors - which in normal circumstances would have been grounds for an editorial review and potential withdrawal.
You can’t make this stuff up. This has so many layers of wrong that it’s hard to find a place to start.
Dr. Wolf went so far as to write a separate editorial in the UHMS Journal (UHMS 2015, Vol. 42, Cognitive Function in a TBI Randomized HBO Trial) stating that both pressure groups improved over baseline, indicating a likelihood of clinical efficacy - contradicting the conclusions of Dr. Cifu - the real author of this sock-puppet paper.
Onto More Drama
On December of 2012, Marty Hoffman was able to set up a meeting with the incoming Surgeon General of the United States Army (December 2011 – December 3, 2015), Lt. Gen. Patricia Horoho. Whealler was associated with the Office of the Surgeon General and was asked by Marty to attend the meeting as a courtesy to inform Lt. Gen. Horoho about the internal resistance by the Army to advancing hyperbaric oxygen for our injured military members. This was to be a private meeting, involving very few people, to share the data that was in the hands of both groups at the time.
The reaction from Whealler was a little over the top. It also showed the level of worry that was being felt by certain groups in the DoD. Heaven-forbid that a treatment with effective results was available! Think of the poor contractors and drug companies!!
Shortly after the meeting was scheduled, Harch’s offices and home started getting phone calls from Whealler, wanting to talk to him, asking for flight numbers, arrival times, where he was staying … you get the picture. Whealler even offered to pick Harch up at the airport. I hope he offered to bring coffee and donuts, too.
With the help of friends that where living in the area, a nondescript little motel was arranged to house Dr. Harch. Marty Hoffman, acting as go between from the airport and motel, provided an extra level of anonymity and security. When both Hoffman and Harch arrived at the Pentagon to the meeting, which was a meeting to share data, Whealler and 12 other people where in the room. An additional group in Texas, on audio hook-up (with a third group somewhere on video) was also awaiting these two men.
Harch and Hoffman were taken aback. This was supposed to be an information exchange for the benefit of the Surgeon General…not a brawl. Both Marty and Paul wisely decided to not engage with them and waited to meet directly with S.G. Lt. Gen. Horoho who was late for the meeting. Harch and Hoffmann first met privately with Horoho and her XO and methodically laid out the sequence of events described above, culminating in Whealler’s contact with the Journal of Neurotrauma’s editor over the publication of the first half of Harch’s veteran’s study. Even Whealler’s attempts to meet/intercept Harch before the Pentagon meeting was provided to General Horoho. This took 30 minutes, during which the other groups waited for the exchange of data meeting. Horoho stoically listened to everything and asked both men to go forward with the scheduled sharing of data. Horoho, Paul and Marty walked into the meeting, Harch opened his computer, and they shared all of the data they had to that point in time. Harch then asked Whealler to review the DoD data. Whealler instructed them that he would be sharing nothing.
Message received…loud and clear.
My Turn Under the Eye
So, it’s at this point that I have my contact with Whealler.
At the time I was in Seattle, an unknown nobody in the field of HBOT. Whealler had come out to Seattle for a conference that was being held in 2012. I was no longer directly involved with HBOT but I wanted to get this therapy approved and for more people to have access to it…therefore I was doing educational lectures to anyone that was willing to listen. I was also a past member of the NBIRR team. Not an important player but a player none the less. Imagine my surprise when I got an email request to meet with Whealler (shock and awe!).
Whealler met me for a coffee. I knew this person by reputation but never met them. I had no knowledge of the previous efforts to suppress important clinical data that were coming from the DoD group and Whealler. The meeting was an awkward conversation, with the good doctor peppering me with questions, trying to extract information on the current NBIRR study, other ongoing projects and my relationship with several researchers on the field of HBOT. I was more than happy to share what I was allowed to share, including the fact that I was convinced of the effectiveness of the therapy.
Whealler then proceeds to divulge that the current study that they are working on (HOPPS - JAMA Intern Med. doi:10.100/jamainternmed.2014.5479) is showing no effect and to be careful with what I could conclude. There was an effort to change my opinion and to dismiss the efforts of people that were actively doing research. The old Jedi Mind Trick was attempted - without much success. The meeting did not last long and we parted ways.
Sidebar 4: Whealler related to me a very disingenuous summary of the results from his HOPPS study. I was shocked to see the published results and was floored by their conclusions. A very clear effect was present when compared to a no-treatment control group. What Whealler and his team basically did was compare the air treatment group (1.3 ATA, air) outcomes to the 100% oxygen (1.5 ATA) outcomes. This is the equivalent of comparing 350 mg of ibuprofen to 650 mg of ibuprofen to determine the effect on headaches. Both doses will work to an equivalent degree. You label the air treatment a placebo (with all the evidence of animal and past-clinical research ignored on pressurized air) and since the differences in outcomes are almost none, you can then declare that there is no difference! Voila - HBOT is no better than the “placebo” - and by a technicality you can declare victory.
Whealler was also present at the Conference where I was presenting that year…paying close attention to what I was saying and being quick to point out that the evidence was not conclusive. Whealler was keeping the Wall of Narrative crack-free - at a regional conference!!
I was glad that we did not meet again.
That sentiment is not due to Whealler being obnoxious or bitchy…Whealler looked like someone who was ordered to keep the story going and was more than willing to do it, even in the face of contradictory data. Just Following Orders.

Getting To The Point
So, we are now in the present, piecing this lost moment of history into a cohesive web of data points. Dr. Harch completed his clinical trial in 2016 and tried to publish in the same journal that published the first half of the trial. The editors wanted nothing to do with it and rejected the manuscript. Looks like the editors got the message - This Is Off-Limits, Stick To The Narrative.
Paul was still able to publish his results (Medical Gas Research, 2017, September, Volume 7, Issue 3) and demonstrated that in the cases of dual diagnosis of TBI (or persistent post-concussion syndrome, PPCS) and PTSD, HBOT helped.
Not by a little.
Not by what the current best standard-of-care treatments could provide.
An order of magnitude better.
Miraculously better.
The conclusion for the report on the first 16 subjects in the Journal of Neurotrauma was that the results, despite no control group in the study, could not be explained by placebo effects. The final paper in Medical Gas Research, with all 30 subjects and a control group for the imaging, was stronger.
Dr. Harch wasn’t the only one to show dramatic effects in recovery. As a matter of fact, several other researchers showed the same or better outcomes. A lot of independent researchers demonstrated clear and large effects in TBI diagnosed patients (across severity scales), including the *Army’s own HBOT clinical trial!
Boussi-Gross et al (2013): PLoS One 2013 Vol. 8 Issue 11 Pages e79995
Rockswold et al (2013): J Neurosurg 2013 Vol. 118 Issue 6 Pages 1317-28
Hadanny et al (2015): Restor Neurol Neurosci 2015 Vol. 33 Issue 4 Pages 471-86
*Miller et al (2015): JAMA Intern Med 2015 Vol. 175 Issue 1 Pages 43-52
Tal et al (2015): Restor Neurol Neurosci 2015 Vol. 33 Issue 6 Pages 943-51
Shandley et al (2017): Undersea Hyperb Med 2017 Vol. 44 Issue 3 Pages 257-269
Tal et al (2017): Front Hum Neurosci 2017 Vol. 11 Pages 508
Hadanny et Al (2018): BMJ Open 2018 Vol. 8 Issue 9 Pages e023387
Weaver et al (2018): Undersea Hyperb Med 2018 Vol. 45 Issue 2 Pages 129-156
Hart et al (2019): Undersea Hyperb Med 2019 Vol. 46 Issue 3 Pages 353-383
Mozayeni et al (2019): Med Gas Res 2019 Vol. 9 Issue 1 Pages 1-12
Harch et al (2020): Med Gas Res 2020 Vol. 10 Issue 1 Pages 8-20
Zhong et al (2020): J Int Med Res 2020 Vol. 48 Issue 10 Pages 300060520939824
Chen et al (2022): Front Neurol 2022 Vol. 13 Pages 929386
Hadanny et al (2022): Sci Rep 2022 Vol. 12 Issue 1 Pages 15233
Liu et al (2023): Medicine (Baltimore) 2023 Vol. 102 Issue 37 Pages e35215
Doenyas-Barak et al (2024): J Clin Psychiatry 2024 Vol. 85 Issue 4
In a May 2024 systematic review of the literature, Drs. Andrews and Harch (Systematic review and dosage analysis: hyperbaric oxygen therapy efficacy in the treatment of posttraumatic stress disorder) established that the evidence level for HBOT is now at “WHY THE FUCK AREN’T YOU USING IT FOR TBI, PCS AND PPCS”.
Those are not their exact words…that’s just my synopsis.
This is what the authors said:
This review provides Centre for Evidence-Based Medicine (3) Class 1 evidence that 40 hyperbaric oxygen treatments at 1.5 ATA oxygen are effective and well-tolerated in mTBI Persistent Post Concussion Syndrome (PPCS). According to the American Society of Plastic Surgeons Grade Practice Recommendations, this evidence meets the threshold for and is a Grade A Practice Recommendation (4).
Both are more scholarly and restrained than I.
But it’s time to get to the bombshell.
The Penny Drops - Big Time
In 2013, at the annual Undersea and Hyperbaric Medical Society meeting, Whealler announced to the gathered members his position as CEO of Nanotherapeutics (2002 - 2017), which is now Ology Bioservices. This company was a contractor for the U.S. Department of Defense, specializing in pharmaceutical research and development, including biodefense and infectious disease treatments. When did Whealler become the CEO of this company? Before, during or after the HOPPS trials? Was this disclosed to the JAMA editors?
The ownership and management details might not be explicitly stated in public records, but the company has historically received substantial contracts from U.S. governmental agencies for medical countermeasures against threats such as infectious diseases and biological warfare agents. Across 20 years, over $500 million in Department of Defense contracts have been awarded to this company. How much over $500 million? Closer to a billion?
Was their R&D being conducted to develop therapies for the treatment of TBI, PPCS or PTSD? That information is not forthcoming. But if there was that sort of research going on, non-disclosure constitutes a conflict of interest. That’s a big no-no.
So, we have Whealler, one of the lead scientists of the HOPPS clinical trial (funded by the DoD/VA/Army) claiming to be the CEO of Nanotherapeutics, Inc. during an active clinical trial, which started in 2011 and published in 2014. The HOPPS paper was a master class in obfuscation, misdirection and just blatant ignoring the facts. It was an absolute dereliction of duty and was coordinated with editorials in JAMA to ensure complete saturation of a single message - WE PROVED THAT HBOT DOES NOT WORK.
Last time I checked, CEOs that manage pharmaceutical companies making $20-$50 million in contracts per year do not help run and manage a clinical trial. Especially if they are active officers in the US Medical Services at the same time - oh, did I forget to mention that little tid-bit? That’s a heavy lift for a simple country CEO.
Whealler was an active duty member of a branch of the armed services - you can’t do both at the same time…unless you are under orders or special consideration.
The conflict-of-interest disclosures that were reported in the JAMA Internal Medicine publication list the following:
Online: Conflict of Interest Disclosures: None reported.
Printed: Conflict of Interest Disclosures: All authors have completed and submitted the ICJME Form for Disclosure of Potential Conflicts of Interest.
Something is not adding up. But it is looking like PhMICkey is in the house.
And if PhMICkey is blocking the use of HBOT, they are committing crimes against their citizens (again). It’s not enough that:
The Tuskegee syphilis experiments took place
NIMH funded and violated patients rights to informed consent (ask Dr. Peter Breggins about that…he’ll tell you)
Clowns-In-America funded MK Ultra/MONARCH/heart attack gun
The COVID19 plan by the DoD/HHS/DHS
God-knows how many other projects (including spraying American citizens with pertussis and other pathogenic bacteria).
A technology that boost one’s own body to accelerate healing and recovery - air & pressure. That is HBOT. A very simple, God-blessed technology.
No fillers, dyes, additives or adulterants.
No intellectual property protections - just the need to meet fire and safety certifications for a pressure vessel. And a good practitioner of the art that can provide a safe treatment.
It works very well and can be dosed for gentle or aggressive interventions.
Add other gases to the mix (argon, helium, xenon) and you can develop some very interesting treatment approaches.
In Summary
So, kids…this is what happens with your taxpayer dollars. Government agencies are working (and funding NGOs) to stop effective treatments from coming forward. Individuals that step out of the curated narrative are targeted for censorship, interference or worse.
This story is only a glimpse into the reach and power that is making Americans sicker, more debilitated and more in debt. Having treatment options that help with recovery from strokes, vascular dementia, Alzheimer’s disease, traumatic brain injury and help reduce recovery time from injuries and surgeries would be a nice option. Oh, and it would save you money.
But we can’t have nice things at a national level.
At least, that’s what our owners are telling us in subtext.
For those that believe themselves to be free, this should be a catalyzing issue. You are not owned and you have every right to have access to effective treatments.
MAHA or Die.
Until next time.
Tell a friend.
(special thanks to Dr. Paul Harch for providing editorial feedback and suggestions)
Wow! I am sadly not surprised. I was a Captain in the Persian Gulf War and involved with the setup of field medical facilities in theater for the USMC. The "state of the art medical supplies" on the prepositioned support ships revealed Vietnam era equipment when received in Saudi Arabia. Woefully outdated yet top dollar had been paid to contractors?! Whistleblowers were treated badly and so it goes on. Thank you for sharing the full picture on HBOT. I hope these criminals get what they deserve.
What an insightful deep dive, Xavier. Thank you. Same old despicable playbook that enriches the immoral greedy people while continuing or causing the suffering of so many of their fellow humans. 😠